
Meniscus: Much more than an important shock absorber

Meniscus, each knee has two. Along the inside of the knee is a moon-shaped sickle, on the outside an open circle. They fulfill 3 functions: pressure distribution, sliding and stability. The inner meniscus carries about 50% of the weight in the knee. The rest rests on the cartilage. The outer one carries even more, namely 70%. The meniscus distributes the weight over a large surface. If you take it away, all the weight presses on the small surface where the cartilage of the femur and tibia meet. The meniscus also allows this cartilage to slide over each other without much resistance. Without menisci, the cartilage scrapes with a very high local peak pressure and that damages the cartilage. In addition, meniscus also contribute to the stability of the knee joint. When an anterior cruciate ligament tears, only the inner meniscus keeps the heads of the femur and lower leg in place in relation to each other when the leg bends. It is exposed to enormous forces and that explains why it wears out so quickly in people who no longer have an anterior cruciate ligament. An excellent educational video can be found here
Partial Meniscectomy

If the meniscus has suffered irreparable damage, the tear is removed during keyhole surgery with special instruments, forceps and shavers. Of course, only the damaged part is removed, the healthy parts are preserved. The partial meniscectomy is the most commonly performed arthroscopic procedure in the world with favorable results in more than 90% of patients. Nevertheless, the risk of further wear of the joint in these patients is increased in the long term (more than 20 years). In a limited number of patients, pain, swelling or accelerated cartilage wear occurs shortly after the procedure. These patients are therefore eligible for additional treatment such as meniscal replacement solutions (see below), osteotomy or even prosthetic surgery.
Degenerative (= wear and tear) meniscus tears often occur after the age of 50 (25%) and should best be treated non-surgically in the first 3 months with physiotherapy, cycling, pain relief and a possible injection. The vast majority of patients will be better after 3 months and will not require surgery. In case of persistent complaints, an arthroscopy and partial meniscectomy can bring relief. A European consensus meeting provides the following guidelines
Meniscus suture
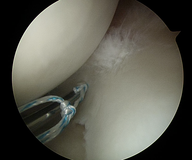
In some cases, a meniscus tear can be repaired with a meniscus suture. Unfortunately, not all tears qualify; only tears in young patients in a well perfused area. During exploratory surgery, the tear is stitched up using advanced repair techniques. The success rates of this operation are about 80%
Save the meniscus when possible: Advanced repair
Meniscus scaffold

Nowadays, we are mainly looking for ways to preserve the meniscus and its function. For example, a scaffold or porous artificial meniscus in which the body's own cells settle and grow into a new meniscus-like structure. For now, this technique is only suitable for partial or smaller painful defects. The operation is done via keyhole surgery. There is currently more than 10 years of experience with this scaffold. The short-term experiences were recently published in the American Journal of Sports Medicine.
Meniscus Transplantation

Young people with pain and a severely damaged or completely removed meniscus, but whose cartilage in the knee is still quite good, are ideal candidates for this meniscus transplant. The entire meniscus is replaced by a donor meniscus, so this technique is intended for larger injuries. The operation is done via keyhole surgery. The disadvantage of meniscus transplantation is of course that a suitable donor meniscus must be available, a waiting list of 6 to 24 months is no longer an exception. We have over 20 years of experience with meniscus transplants which has been published in all leading orthopedic journals
Meniscus Protheseis

This innovative technique is now available but is not yet reimbursed. This polyurethane artificial meniscus is a solution for somewhat older people where the inner or medial meniscus had to be largely removed. In this case, the worn meniscus is then replaced by a plastic meniscus prosthesis. More information can be found here!